
From the 1Academic Department of Rehabilitation Medicine, University of Leeds, 2National Demonstration Centre for Rehabilitation Medicine, Leeds Teaching Hospitals NHS Trust, 3Leeds Community Healthcare NHS Trust, 4NHS Leeds Clinical Commissioning Group, 5Critical Care Medicine, Leeds Teaching Hospitals NHS Trust, 6Bradford District Clinical Commissioning Group and 7Respiratory Medicine, Leeds Teaching Hospitals NHS Trust, Leeds, UK
Objective: COVID-19 is a multisystem illness with considerable long-term physical, psychological, cognitive, social and vocational sequelae in survivors. The aim of this study is to describe the development of an integrated rehabilitation pathway using tele-medicine approach to manage these sequelae in a systematic and efficient way.
Methods: A multidisciplinary team of professionals used a consensus method to define pathway referral criteria based on the COVID-19 Yorkshire Rehabilitation Screen (C19-YRS) telephone screening tool developed previously by the team. Specialists needed for the pathway to operate were also decided.
Results: A rehabilitation pathway, which spans the acute hospital trust, community trust and primary care service within the UK National Health Service (NHS) service model was developed. C19-YRS referral criteria thresholds for informing the decision making process were defined. A dedicated multidisciplinary COVID-19 rehabilitation team is responsible for dealing with the management of complex cases with needs spanning across multiple domains of the health condition.
Conclusion: An integrated COVID-19 rehabilitation pathway based on our previously published C19-YRS tool is proposed. Future research is needed for validation of the pathway. We recommend health services dealing with the pandemic to adopt such a pathway to manage the care of the COVID-19 survivors in the community.
Key words: C19-YRS; telephone screening tool; long-term; hospital.
Accepted Aug 11, 2020; Epub ahead of print Aug 6, 2020
J Rehabil Med 2020; 52: jrm00089
Correspondence address: Manoj Sivan, Academic Department of Rehabilitation Medicine, D Floor, Martin Wing, Leeds General Infirmary, Leeds, LS1 3EX, UK. E-mail: M.Sivan@leeds.ac.uk
COVID-19 can cause considerable physical, mental, cognitive, social and vocational problems that persist for a long time in those who survive the illness. Given the scale of this burden and lockdown measures in most countries, there is a need for an efficient healthcare system for identifying individual’s needs and directing them to relevant rehabilitation services. Based on the nature and severity of symptom (s) on a previously developed telephone screening tool, the COVID-19 Yorkshire Rehabilitation Screen (C19-YRS), specific referral criteria for services have been developed in this study. Specialists needed for the rehabilitation services in the system are also described. The authors recommend that health services across the globe dealing with the pandemic adopt such a novel integrated rehabilitation system in order to manage the large number of COVID-19 survivors in an effective manner.
To date, the COVID-19 pandemic has infected more than 13 million people worldwide, with more than 578,000 deaths. The majority (>80%) of cases have a mild presentation, either with no symptoms or with mild upper respiratory tract infection symptoms (1). Approximately 14% of cases develop severe disease within 24–48 h, with dyspnoea, increased respiratory rate, hypoxia and/or lung infiltrates, needing hospitalization (1). A small, but significant, minority of cases (5%) develop critical disease with respiratory failure, septic shock and/or multiple organ dysfunction/failure, needing management in intensive care units. The case fatality rate has been reported as between 2% and 10% in different countries, depending on the extent of test-ing and reporting of deaths due to the illness (2, 3).
Whilst usually presenting as a respiratory infection, it is now known that COVID-19 is truly a multi-system illness with common complications affecting the respiratory system (acute respiratory distress syndrome, pulmonary embolism), musculoskeletal (weakness, pain, fatigue), cardiac (arrhythmias, myocardial injury), renal (acute kidney injury), gastrointestinal, nervous (neuropathy, encephalopathy) and endocrine systems (4). The short- and long-term sequelae for survivors (including those discharged from hospital care) are currently unknown, but reports are starting to emerge on their symptoms and needs (5, 6). Post-illness fatigue, breathlessness and psychological problems, including post-traumatic stress disorder (PTSD), anxiety and depression are reported in approximately one-third of survivors, even at 7 weeks after discharge from hospital. Long-term symptoms (beyond 6 months) can be predicted, based on problems seen in previous coronavirus outbreaks (7).
The UK NHS Long Term Plan (2019) published before the COVID-19 pandemic pledges to improve outcomes for people with serious conditions by investing in out-of-hospital care and community services (8). The emphasis is on providing personalized digitally-enhanced care that can be sustained long-term. Given the scale of post- COVID-19 problems long-term in the community, there is a need for a comprehensive screening for post-discharge symptoms and an integrated rehabilitation pathway to optimally manage these individuals (9). This study describes applying referral criteria thresholds to a previously developed telephone screening tool, in order to direct individuals to the best possible health service and enable a seamless management pathway across primary, secondary and tertiary care.
Leeds Teaching Hospitals NHS Trust (LTHT) is one of the largest hospital trusts in Europe with approximately 1800 beds and providing secondary and tertiary services to a population of 2.5 million people in the region. Patients treated for COVID-19 after discharge are followed up members a multidisciplinary team comprising of physiotherapists, occupational therapists (OT), dietitians, speech and language therapists (SLT), neuropsychologists and physicians in rehabilitation medicine, respiratory medicine or intensive care. The team previously developed a telephone screening tool along with rehabilitation specialists of Airedale and Hull NHS Trusts (10).
The C19-YRS screening tool
This tool was developed especially to screen individuals recovering from COVID-19 in the community for symptoms using a telephone consultation (10). It also enables scoring the severity of the symptom and its impact on functioning. The symptoms covered by the tool are breathlessness, voice, swallowing, nutrition, mobility, fatigue, personal care, usual activities, pain/discomfort, anxiety, depression, post-traumatic stress disorder, continence, cognition, perceived health status and family/carers views.
There are 19 questions capturing the main symptoms (spanning across all WHO ICF domains), each with either yes/no response options or a 0-10 numerical rating scale grading the impact of that symptom on their functioning. The patient is also asked to provide a response for each symptom pre-illness (pre-COVID-19) if possible (this is not mandatory and will be difficult for those with cognitive impairment). The tool also captures medical problems since discharge, utilisation of healthcare services including re-admission to acute care hospital, and family members’ perspectives on impact of the illness. It is administered by a specialist clinician who is qualified and suitably trained to provide advice and suggestions to the patient during the telephone call. The tool takes approximately 15 minutes to administer.
In this study, the Leeds multidisciplinary team used a consensus method to develop referral criteria that can be applied to the C19-YRS tool to determine management of individuals in appropriate rehabilitation services. The services described in the pathway were either existing rehabilitation services or new services identified to manage complex post-COVID cases which the team felt could not be managed by existing services. The focus has been to develop community based rehabilitation through the collaboration of acute, community and primary care providers, facilitated by commissioners for healthcare services in the region.
COVID rehabilitation pathway and referral thresholds
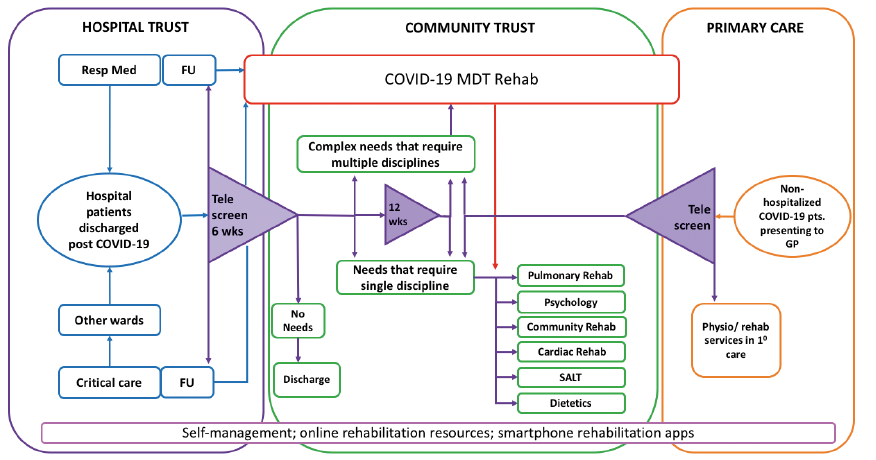
Clinicians caring for individuals at various points in the COVID rehabilitation pathway can use the C-19 YRS screening tool to capture ongoing symptoms. In secondary care this screening is performed by the specialist team following up discharged patients. In primary care the primary care clinician or general practitioner (GP) administers the tool. Fig. 1 and Table I summarize the pathway and criteria for triggering referrals for the services within the healthcare system.
Fig. 1. COVID-19 rehabilitation pathway showing nodal points of telephone screening and links to rehabilitation services. Resp Med: respiratory medicine; FU: follow-up; SALT: speech and language therapist; MDT: multidisciplinary team; 10: primary; GP: general practitioner.
Table I. Threshold criteria in the COVID-19 Yorkshire Rehabilitation Screen (C19-YRS) telephone screening tool for ongoing referrals. First screen: 6 weeks post-discharge. Follow-up screen 12 weeks post-discharge, when required
The COVID-19 integrated rehabilitation pathway developed in this study provides a potentially effective model for MDT follow-up in the community, in line with the UK NHS long term plan (8). The basis of the pathway is to remotely assess the individuals and direct them to the most appropriate rehabilitation service. The telephone screening tool (C19-YRS) remains the nodal point of the pathway networks and is applied either at 6 and 12 weeks post-discharge for hospitalized individuals or administered in primary care for individuals who did not need hospitalization whenever they present to the GP. The tool enables prompt detection of post-discharge symptoms referral to specialist services/professionals based on needs. If individuals are improving and prefer to continue with self-management measures, they will continue to be monitored and will be contacted again for a subsequent screening consultation after approximately 6 weeks.
Several self-help educational resources have been developed to help support individuals recovering from COVID-19. NHS England plans to publish a national online resource, ”Your COVID Recovery” shortly (11). The Lancashire Teaching Hospitals NHS Trust online resource provides strategies for pulmonary rehabilitation and optimization of physical and mental health (12). Similar resources are available for those with psychological issues, such as low mood, anxiety and stress (13). Clinicians might also use a combination of targeted therapy and self-help resources to optimize interventions to individual needs.
The role of the professionals needed to look after these individuals long-term in these pathways are shown in Table II. The pathway co-ordinator is a qualified clinician coordinating the care across services, and and presents any complex cases to the C19-MDT for troubleshooting. Complexity is defined as symptoms of a severe nature in at least 2 health domains or mild/moderate symptoms in 3 health domains (Table I). The MDT must have the expertise to perform a detailed work-up of the individual and provide targeted interventions either via a face-to-face appointment with appropriate personal protective equipment (PPE) or using remote tele-consultation methods, or a combination of both modes of service delivery. The management plan of the C19-MDT can include referral to individual services for specific programmes, such as pulmonary rehabilitation or fatigue management.
Table II. Role of professionals involved in the pathway
The C19-MDT will have specialist input from hospital experts, such as respiratory medicine and cardiology, to provide opinion and cascade the care back to the hospital for urgent investigations and management. One of the challenges in the follow-up of COVID-19 patients is that the natural history and course of recovery of the condition are unclear, and experience is relatively limited. Therefore, any follow-up and rehabilitation pathway must include as many specialists as possible and be able to adapt to individual needs as they arise. For example, the symptom of breathlessness may require acute intervention due to concern regarding pulmonary embolism, or a longer term approach due to issues of post-infective fibrotic changes.
Rehabilitation interventions provided to individuals recovering from COVID-19 can be delivered using remote audio/video consultations (tele-rehabilitation) (14). Zhao et al., in their recommendations for pulmonary rehabilitation for COVID-19 patients in the community, suggest the use of educational videos, instruction manuals, or remote consultation (15). Telemental health services have been used to provide psychological support, supervision and training, not only for people recovering from COVID-19, but also for the general population at high risk of mental health problems during the pandemic (16, 17).
Outcomes measures can be administered at various service entry and exit points, in order to capture changes in health condition and the effect of the interventions. The C19-YRS tool is a screening tool and not an outcome measure on its own. However, given that it captures the severity of symptoms and health status on a grading Likert scale, these aspects can be monitored over time when individuals have repeated screening. Outcome measures, when selected, should span all domains of the health condition, using the WHO ICF framework to select suitable measures.
There are some limitations to the COVID rehabilitation pathway described in this study. The nature of the healthcare services described is typical of the NHS in the UK. However, the authors believe that most countries have approximately a 3-tier system (primary, secondary and tertiary care), and that the approach and tools described in this paper are applicable to most countries. In addition, clinicians worldwide may already be using their own comprehensive assessment checklists, which may be similar to the C19-YRS tool.
In summary, a pragmatic, simple, comprehensive and integrated rehabilitation pathway was developed to screen COVID-19 survivors and target specific rehabilitation interventions in a timely and efficient manner, based on the screening tool C19-YRS. This is intended as a framework that can be adapted easily to suit local service needs and priorities in any country affected by COVID-19. Future research will explore the effectiveness and cost-efficiency of such structured pathways.
The authors would like to thank all the members of the Leeds COVID-19 multidisciplinary rehabilitation team, clinicians in primary and secondary care and commissioners who provided valuable input to the development of the pathway described in this study.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize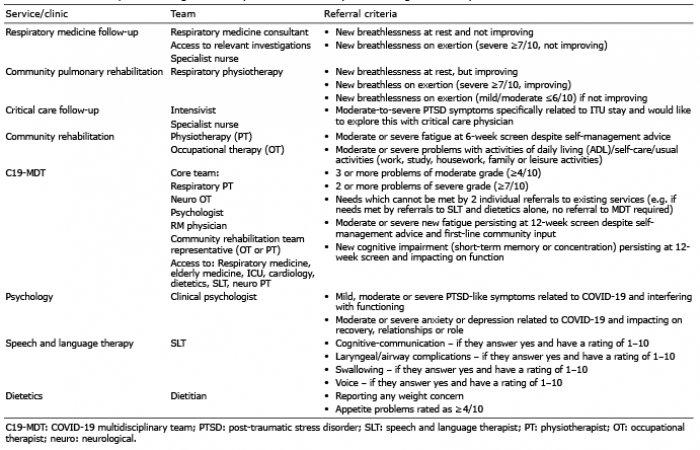 Click to show fullsize
Click to show fullsize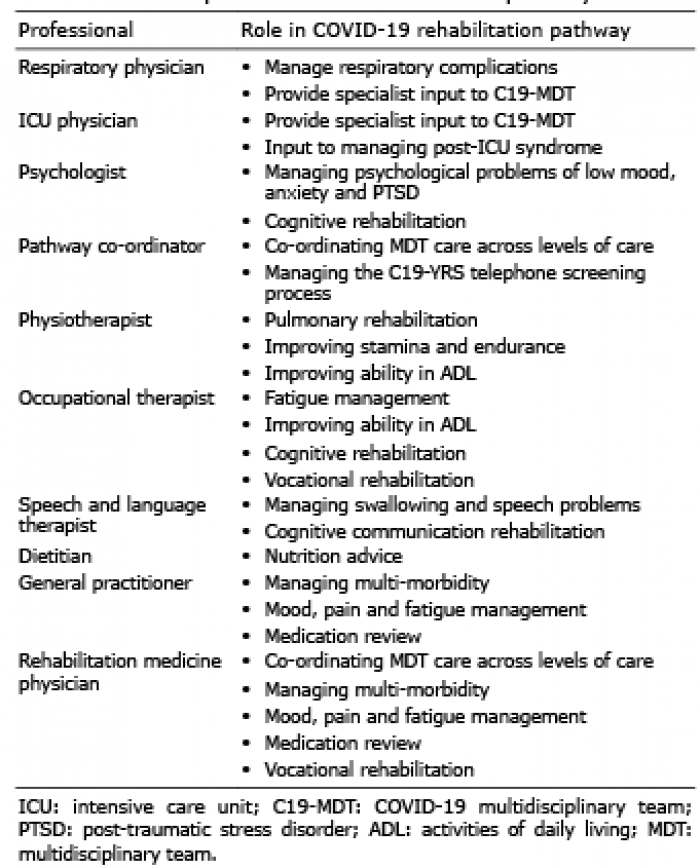 Click to show fullsize
Click to show fullsize